The HRSA Women’s Health USA 2011, the 10th edition of an annual data book identifying priorities, trends, and disparities in women’s health, is now available. The 2011 edition highlights several new topics, including secondhand tobacco smoke exposure, Alzheimer’s disease, preconception health, unintended pregnancy, oral health care utilization, and barriers to health care. For the first time, the special population section of the report features data on the health of lesbian and bisexual women, as well as Native Hawaiian and other Pacific Islander women. Data on American Indian and Alaska Native women are also featured.
Press Release: http://www.hrsa.gov/about/news/pressreleases/111031womenshealth.html
Reposted at http://www.darkestcloset.blogspot.com/
Thursday, December 29, 2011
Friday, December 23, 2011
Three Recent Articles Describe Recovery-Oriented Approaches
Behavioral Healthcare recently published a two-part interview with author Robert Whitaker as well as an article about the Hearing Voices Network; and The New York Times ran an article highlighting the importance of peer support. The two-part Whitaker interview – by Bill Anthony, Ph.D., and Lori Ashcraft, Ph.D. – covers Whitaker’s thoughts about the effectiveness of psychotropic medications (among other topics) and includes a sidebar from a critic of his views.
Said Whitaker, “. . . [U]nfortunately I’m afraid psychiatry no longer knows how to get back on track with honest reporting of what it does and does not know, and honest investigations of psychiatric medications. . . . Ultimately, I think we need a new paradigm built on the framework of psychosocial and recovery practices.” The Hearing Voices Network story, published online, covers a presentation by Daniel Hazen, executive director of Voices of the Heart Inc., and Oryx Cohen director of the National Empowerment Center Technical Assistance Center. They offered strategies for handling the experience of hearing voices. “The notion that peer-led groups might help voice-hearers to tame and better live with their voices was, in the words of one local psychiatrist, ‘liberating,’ ” Behavioral Healthcare reported.
The New York Times article featured the story of Antonio Lambert, diagnosed with bipolar disorder and a co-occurring substance use disorder, who was sentenced to 22 years in prison when he was 17 years old. Today, Antonio trains peer specialists across the United States. The article – the last of a five-part series entitled “Restoring Lives,” about individuals with psychiatric diagnoses who are in recovery – quoted Larry Davidson of Yale University: “Peers are living, breathing proof that recovery is possible, that it is real.”
Sources: http://www.behavioral.net/ME2/dirmod.asp?sid=9B6FFC446FF7486981EA3C0C3CCE4943&nm=Archives&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=A5BC331586DC4D8B89B194044A0D83F1
http://www.behavioral.net/ME2/dirmod.asp?sid=9B6FFC446FF7486981EA3C0C3CCE4943&nm=Archives&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=43C2D89CC0364CFA94916B05462A9556#sidebar
http://www.behavioral.net/ME2/dirmod.asp?sid=&nm=&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=2AD887EA1E4847C293174A191EAEA422
http://www.nytimes.com/2011/12/20/health/20lives.html?ref=health">http://www.nytimes.com/2011/12/20/health/20lives.html?ref=health
Reposted at http://www.darkestcloset.com/
Said Whitaker, “. . . [U]nfortunately I’m afraid psychiatry no longer knows how to get back on track with honest reporting of what it does and does not know, and honest investigations of psychiatric medications. . . . Ultimately, I think we need a new paradigm built on the framework of psychosocial and recovery practices.” The Hearing Voices Network story, published online, covers a presentation by Daniel Hazen, executive director of Voices of the Heart Inc., and Oryx Cohen director of the National Empowerment Center Technical Assistance Center. They offered strategies for handling the experience of hearing voices. “The notion that peer-led groups might help voice-hearers to tame and better live with their voices was, in the words of one local psychiatrist, ‘liberating,’ ” Behavioral Healthcare reported.
The New York Times article featured the story of Antonio Lambert, diagnosed with bipolar disorder and a co-occurring substance use disorder, who was sentenced to 22 years in prison when he was 17 years old. Today, Antonio trains peer specialists across the United States. The article – the last of a five-part series entitled “Restoring Lives,” about individuals with psychiatric diagnoses who are in recovery – quoted Larry Davidson of Yale University: “Peers are living, breathing proof that recovery is possible, that it is real.”
Sources: http://www.behavioral.net/ME2/dirmod.asp?sid=9B6FFC446FF7486981EA3C0C3CCE4943&nm=Archives&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=A5BC331586DC4D8B89B194044A0D83F1
http://www.behavioral.net/ME2/dirmod.asp?sid=9B6FFC446FF7486981EA3C0C3CCE4943&nm=Archives&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=43C2D89CC0364CFA94916B05462A9556#sidebar
http://www.behavioral.net/ME2/dirmod.asp?sid=&nm=&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=2AD887EA1E4847C293174A191EAEA422
http://www.nytimes.com/2011/12/20/health/20lives.html?ref=health">http://www.nytimes.com/2011/12/20/health/20lives.html?ref=health
Reposted at http://www.darkestcloset.com/
" Boycott Normal” – May 5, 2012, in Philadelphia
On May 5, 2012, MindFreedom International will hold a march and rally in Center City Philadelphia to coincide with the American Psychiatric Association (APA) annual meeting, at which the new version of the Diagnostic and Statistical Manual, DSM-5, is scheduled to be rolled out prior to its 2013 release. “Raise your voices for more non-drug choices!” is one of the rallying cries for the event. See the source below for ways to participate:
Source: http://www.mindfreedom.org/campaign/boycott-normal/boycott-more-info
Source: http://www.mindfreedom.org/campaign/boycott-normal/boycott-more-info
Copeland Center Publishes Position Paper on Seclusion and Restraint
Copeland Center Publishes Position Paper on Seclusion and Restraint
The Copeland Center for Wellness and Recovery has published a position paper calling for the elimination of seclusion and restraint, both physical and chemical. “The paper also aspires to stimulate an active and ongoing dialogue about alternatives to seclusion and restraints among change agents in the mental health recovery arena. . . . The Center also opposes the use of body bags of any kind, strait jackets and other devices that restrict movement, full body searches including body cavity searches, torture of any kind, the use of tasers and the use of force or coercion as treatment for emotional distress.The Center believes the use of these methods in any area of psychiatric services should be prohibited by national and international law.” The Center is developing an action plan to work toward achieving these goals. The paper is available at the following link:
http://tinyurl.com/copeland-sr-position
Source: http://www.copelandcenter.com Reposted at http://www.darkestcloset.blogspot.com/,
CASD Publishes Fourth in a Series of Research & Practice Briefs
A paper on barriers and incentives to finding employment as perceived by individuals with psychiatric disabilities has been published by the Center on Adherence and Self-Determination (CASD). The paper also investigates the relationship between incentives and commitment to obtaining employment, as well as the use of motivational interviewing to help people improve employment outcomes. The paper is available at the source below.
Source: http://www.adherenceandselfdetermination.org/images/stories/casdrpb112011.pdf
Reposted at http://www.darkestcloset.blogspot.com/,
Source: http://www.adherenceandselfdetermination.org/images/stories/casdrpb112011.pdf
Reposted at http://www.darkestcloset.blogspot.com/,
CMS Finds Overpayment for Antipsychotic Medications
Physicians too often violate federal standards designed to prevent overmedication and inappropriate use of drugs, according to a report by the Office of the Inspector General of the U.S. Department of Health and Human Services.
Testifying before a U.S. Senate panel recently, high-ranking government officials said that in the six months between Jan. 1 and June 30, 2007, 51 percent of the Medicare reimbursement claims for atypical antipsychotic medications were erroneous and cost the program $116 million. The report also found that 83 percent of all reviewed Medicare atypical antipsychotic drug claims for older adults living in nursing homes were for off-label uses. The officials said that more care must be taken to keep physicians from prescribing such medications, although the panel’s chairman noted that the drugs can be beneficial “when properly prescribed,” according to an article published in Health Care Daily Report.
Source: http://www.bna.com/officials-antipsychotic-drug-n12884904634/
Reposted htttp://www.darkestcloset.com
Testifying before a U.S. Senate panel recently, high-ranking government officials said that in the six months between Jan. 1 and June 30, 2007, 51 percent of the Medicare reimbursement claims for atypical antipsychotic medications were erroneous and cost the program $116 million. The report also found that 83 percent of all reviewed Medicare atypical antipsychotic drug claims for older adults living in nursing homes were for off-label uses. The officials said that more care must be taken to keep physicians from prescribing such medications, although the panel’s chairman noted that the drugs can be beneficial “when properly prescribed,” according to an article published in Health Care Daily Report.
Source: http://www.bna.com/officials-antipsychotic-drug-n12884904634/
Reposted htttp://www.darkestcloset.com
Facebook Provides First-of-Its-Kind Service to Help Prevent Suicides
In partnership with the National Action Alliance for Suicide Prevention, Facebook has announced a new service attempting to prevent suicides across North America. The service enables Facebook users to report a suicidal comment posted by a friend using either the Report Suicidal Content link https://www.facebook.com/help/contact.php?show_form=suicidal_content or the links found throughout the site.
The poster of the comment will immediately receive an e-mail from Facebook encouraging them to call the National Suicide Prevention Lifeline http://www.suicidepreventionlifeline.org at 1-800-273-TALK (8255) or to click on a link to begin a confidential chat with a crisis worker. The project is a collaboration among the Substance Abuse and Mental Health Services Administration (SAMHSA), the National Suicide Prevention Lifeline and Facebook.
In another story, a new survey by University of Washington researchers has found that, while about one of nine youths attempt suicide by the time they graduate from high school, nearly 40 percent of those who said they had tried suicide reported their first attempt was before they entered high school. The study was published in the November issue of the Journal of Adolescent Health http://jahonline.org/article/S1054-139X(11)00127-3/abstract.
Sources: http://www.samhsa.gov/newsroom/advisories/1112125820.aspx
http://www.nlm.nih.gov/medlineplus/news/fullstory_119226.html
The poster of the comment will immediately receive an e-mail from Facebook encouraging them to call the National Suicide Prevention Lifeline http://www.suicidepreventionlifeline.org at 1-800-273-TALK (8255) or to click on a link to begin a confidential chat with a crisis worker. The project is a collaboration among the Substance Abuse and Mental Health Services Administration (SAMHSA), the National Suicide Prevention Lifeline and Facebook.
In another story, a new survey by University of Washington researchers has found that, while about one of nine youths attempt suicide by the time they graduate from high school, nearly 40 percent of those who said they had tried suicide reported their first attempt was before they entered high school. The study was published in the November issue of the Journal of Adolescent Health http://jahonline.org/article/S1054-139X(11)00127-3/abstract.
Sources: http://www.samhsa.gov/newsroom/advisories/1112125820.aspx
http://www.nlm.nih.gov/medlineplus/news/fullstory_119226.html
SAMHSA Releases New Working Definition of Recovery
Reposted at http:/www.darkestcloset.bloggerspot,
SAMHSA recently announced a new working definition of recovery from mental disorders and substance use disorders. The definition is the product of a year-long effort by SAMHSA and a wide range of partners in the behavioral health care community and other fields to develop a working definition of recovery that captures the essential, common experiences of those recovering from mental disorders and substance use disorders. Major guiding principles support the recovery definition. SAMHSA led this effort as part of its Recovery Support Strategic Initiative.
The new working definition of Recovery From Mental Disorders and Substance Use Disorders is as follows:A process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential.
Through the Recovery Support Strategic Initiative, SAMHSA also has delineated four major dimensions that support a life in recovery:- Health: Overcoming or managing one's disease(s) as well as living in a physically and emotionally healthy way.
- Home: A stable and safe place to live.
- Purpose: Meaningful daily activities, such as a job, school, volunteerism, family caretaking, or creative endeavors, and the independence, income, and resources to participate in society.
- Community: Relationships and social networks that provide support, friendship, love, and hope.
Friday, December 2, 2011
Circle of Friends Key to Adopting Healthy Habits: Study
When people of similar age, sex, size buddied up online, they made gains, researchers say
By Maureen Salamon
THURSDAY, Dec. 1 (HealthDay News) -- Interested in adopting healthier habits? You have a better chance of success if you find a friend with similar traits to share the experience, a new study suggests.
Participants paired with others of similar body mass, age, fitness level and diet preferences were three times as likely to adopt healthy behaviors as those matched randomly in an Internet-based study conducted by a researcher from the Massachusetts Institute of Technology (MIT).
"I think the reality is, we as individuals may have less motivation to change on our own than if we're surrounded by our peer group, even if we met on a social network site," said Dr. Victor Fornari, director of child and adolescent psychiatry at North Shore-LIJ Health System in New Hyde Park, N.Y., who is familiar with the study. "We're very influenced by the group phenomenon."
The study is published in the Dec. 2 issue of the journal Science.
For the study, an online social network was created to promote health and fitness. Broken into small groups of "health buddies," 710 participants were introduced to the idea of an online diet diary through a "dummy" participant who invited others to take part. Each participant was provided with a personalized, online "health dashboard" that displayed real-time information, such as daily exercise minutes, healthy behaviors and personal characteristics of the health buddies.
At the end of seven weeks, those who were matched with health buddies using the principle of "homophily" -- the tendency of people to have similar friends -- were far more likely to use the diet diary and take part in other healthy behaviors than participants whose buddies were assigned randomly. Not one obese individual signed up for the diet diary in the random networks, compared to more than 12 percent of obese participants in the similarly matched networks.
The results also suggest that the most effective social environment for increasing the willingness of obese people to adopt a behavior is one where they interact with others with similar health characteristics, the study said.
"I think it was a pretty brilliant study," said Tricia M. Leahey, an assistant professor of psychiatry and human behavior at the Warren Alpert Medical School of Brown University and Miriam Hospital's Weight Control and Diabetes Research Center in Providence. "It's neat that they're actually starting to manipulate a social network in a way specific to homophily."
Group therapy is also partially based on the premise that people can empathize better with others they relate to, said Dr. Alan Manevitz, a clinical psychiatrist at Lenox Hill Hospital in New York City.
"The question of whether people can benefit from role models that show how to move out of similar thinking is also part and parcel of the development of social networks," Manevitz said. "We all need to be able to interact with people who can promote other senses of self, that you can take in and create within yourself."
However, the current findings refute prior research. Leahey wrote a study published in January 2011 that indicated that overweight people tend to have more social contacts who are also overweight or obese.
"We can say, 'Gee, if I'm in a network of relatively healthy individuals and become friends with someone who's overweight or obese, we might be influenced by this one individual,'" she said. "So I guess it cuts both ways."
But Leahey said she has observed results similar to the new study in "Shape Up RI," a statewide initiative in Rhode Island that draws friends, family members and coworkers into teams to increase exercise, family meals, fruit and vegetable consumption and reduce screen time. The program has shown that group support can become a powerful driver of healthy behaviors, she said.
Ideally, Fornari and Leahey said, the findings should spur other statewide or public programs promoting healthy lifestyles either in person or on Internet-based social networks.
"Certainly, that would be an exciting opportunity and I know that more and more educational opportunities will be web-based," Fornari said.
More information
For more about healthy behaviors, see the U.S. National Library of Medicine.
SOURCES: Tricia M. Leahey, Ph.D., assistant professor, psychiatry and human behavior, Warren Alpert Medical School of Brown University and Miriam Hospital's Weight Control and Diabetes Research Center, Providence; Victor Fornari, M.D., director, child and adolescent psychiatry, North Shore-LIJ Health System, New Hyde Park, N.Y.; Alan Manevitz, M.D., clinical psychiatrist, Lenox Hill Hospital, New York City; Dec. 2, 2011, Science
Last Updated: Dec. 01, 2011
Copyright © 2011 HealthDay. All rights reserved
Tuesday, November 29, 2011
Ricky Wyatt, Lead Plaintiff in Important Class Action Lawsuit, Has Died
Ricky Wyatt, a 57-year-old Alabama man who was the lead plaintiff in a 1970 federal class-action lawsuit that helped improve conditions in state psychiatric institutions nationwide, died on November 1. Wyatt had been institutionalized at age 14 on the word of his legal guardian, an aunt, because he was a “hell-raiser” (as he later described himself). Despite having no mental health diagnosis, he was routinely dosed with Thorazine and other psychiatric medications, and lived in horrendous conditions in Bryce State Hospital in Tuscaloosa. The lawsuit, Wyatt v. Stickney, resulted in national guidelines called the Wyatt Standards; the standards called for a humane psychological and physical environment, qualified and sufficient staff, individualized treatment plans and minimum restriction of patient freedom.
Source: http://www.nytimes.com/2011/11/04/health/ricky-wyatt-57-dies-plaintiff-in-landmark-mental-care-suit.html
Reposted at http://www.darkestcloset.blogspot/
Source: http://www.nytimes.com/2011/11/04/health/ricky-wyatt-57-dies-plaintiff-in-landmark-mental-care-suit.html
Reposted at http://www.darkestcloset.blogspot/
Monday, November 14, 2011
With the Help of a Video Game, Virtual Help for Families of Veterans
Friday, November 11, 2011 By Fred Mogul Click to play
Posted at http://www.darkestcloset.blogspot.com/,
- Christian Campos (Fred Mogul/WNYC)

Christian Campos is playing a different kind of video game.
Campos, 25, has been following the animated story of a U.S. Marine who has returned home to live with his parents after serving on the front lines.
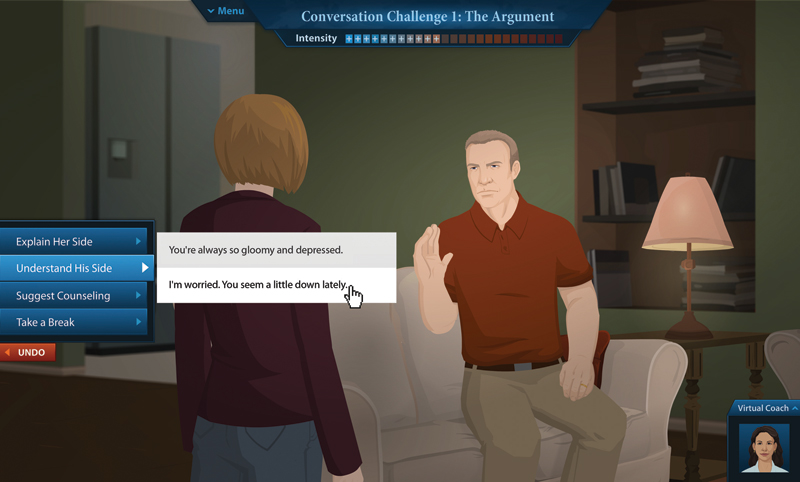
The game, “Family of Heroes,” is an online interactive role-playing program aimed at helping loved ones communicate with veterans dealing with post-deployment problems, and ultimately, get them treatment.
He nodded his head and smiled knowingly at the screen. He said the similarities between the fictional Marine and his brother, Junior, 22, were uncanny.
Junior spent 10 months in Afghanistan and earlier this year returned to Camp Lejeune, N.C., where he is now. He’s come home to his family in Paterson, N.J., a few times since being back.
“Seeing my brother very anxious, seeing my brother with all those feelings of going back to war, because be feels more safe, he feels more normal, he feels he belongs there — is totally sad, is totally devastating to me as well as my parents," Christian said.
There are an estimated 34,000 veterans of the Afghanistan and Iraq wars in the metropolitan area, and with the final withdrawal of troops from Iraq by the end of the year, that number is expected to increase. As many as two-thirds of combat veterans locally have mental health problems, including anxiety, depression, substance abuse and post-traumatic stress disorder, according to the Veterans Administration.
(Photo: Courtesy of Kognito Interactive)
The military services, the V.A. and independent support groups offer a range of services for families, so they can get help for their loved ones, but many people don’t know where to start.
Ann Feder, a supervisor for mental health services for the regional V.A., hopes the new online program that Christian Campos is playing, called Family of Heroes, will find its way to other people like the Campos family.
“We already do face-to-face outreaches,” she said, “but this is the first time we’re doing a program for any family member, loved one, somebody who cares about the veteran online.”
"Family of Heroes" was produced by a New York City firm called Kognito, which has a $200,000 contract with the local V.A. It's too new to have much of a track record, but more rigorous study is in the works.
V.A. officials said they don’t expect an interactive online program to take the place of traditional resources for families, such as help lines and support groups.
Psychologist Barbara Van Dahlen, who runs a volunteer program for veterans called Give an Hour, said the easy-to-access simulation is one more tool among several.
“Obviously, it’s not going to be the right method for every family,” Van Dahlen said. “But the goal is to create a variety of options, of opportunities to get information to families.”
"Family of Heroes" takes about an hour, and features three families with different challenges. Viewers watch a conversation between spouses or parents and returning veterans, and then replay it, taking the role of the loved one, and trying out different replies, until gently persuading the veteran to seek counseling help.
Christian Campos, taking the role of the virtual Marine’s mother, doesn’t quite get him all the way into therapy, but playing around just a little with the simulation, he gets him to accept the idea of possibly seeing someone. It’s a start.
Christian said he feels newly confident about broaching sensitive subjects with his brother, Junior, who’s returning soon for Thanksgiving: “Knowing how to handle a situation...that could save his life,” Christian said.
Christian Campos said his brother, Junior, was in several vehicles that were hit by roadside bombs, and he was shot in the head, but saved by his helmet.
Speaking from North Carolina, Junior said coming back from Afghanistan took some adjustment initially. He had some problems with anger, but not any more.
“I have no issues. I have no problems now,” he said. “I can control my temper now. I’m calm all the time.”
Junior’s looking forward to coming home for Thanksgiving. Christian, is also upbeat about the upcoming visit – but he also plans to spend some time with the “Family of Heroes” program, and go over it with his parents, just in case.
The game, “Family of Heroes,” is an online interactive role-playing program aimed at helping loved ones communicate with veterans dealing with post-deployment problems, and ultimately, get them treatment.
He nodded his head and smiled knowingly at the screen. He said the similarities between the fictional Marine and his brother, Junior, 22, were uncanny.
Junior spent 10 months in Afghanistan and earlier this year returned to Camp Lejeune, N.C., where he is now. He’s come home to his family in Paterson, N.J., a few times since being back.
“Seeing my brother very anxious, seeing my brother with all those feelings of going back to war, because be feels more safe, he feels more normal, he feels he belongs there — is totally sad, is totally devastating to me as well as my parents," Christian said.
There are an estimated 34,000 veterans of the Afghanistan and Iraq wars in the metropolitan area, and with the final withdrawal of troops from Iraq by the end of the year, that number is expected to increase. As many as two-thirds of combat veterans locally have mental health problems, including anxiety, depression, substance abuse and post-traumatic stress disorder, according to the Veterans Administration.
(Photo: Courtesy of Kognito Interactive)
The military services, the V.A. and independent support groups offer a range of services for families, so they can get help for their loved ones, but many people don’t know where to start.
Ann Feder, a supervisor for mental health services for the regional V.A., hopes the new online program that Christian Campos is playing, called Family of Heroes, will find its way to other people like the Campos family.
“We already do face-to-face outreaches,” she said, “but this is the first time we’re doing a program for any family member, loved one, somebody who cares about the veteran online.”
"Family of Heroes" was produced by a New York City firm called Kognito, which has a $200,000 contract with the local V.A. It's too new to have much of a track record, but more rigorous study is in the works.
V.A. officials said they don’t expect an interactive online program to take the place of traditional resources for families, such as help lines and support groups.
Psychologist Barbara Van Dahlen, who runs a volunteer program for veterans called Give an Hour, said the easy-to-access simulation is one more tool among several.
“Obviously, it’s not going to be the right method for every family,” Van Dahlen said. “But the goal is to create a variety of options, of opportunities to get information to families.”
"Family of Heroes" takes about an hour, and features three families with different challenges. Viewers watch a conversation between spouses or parents and returning veterans, and then replay it, taking the role of the loved one, and trying out different replies, until gently persuading the veteran to seek counseling help.
Christian Campos, taking the role of the virtual Marine’s mother, doesn’t quite get him all the way into therapy, but playing around just a little with the simulation, he gets him to accept the idea of possibly seeing someone. It’s a start.
Christian said he feels newly confident about broaching sensitive subjects with his brother, Junior, who’s returning soon for Thanksgiving: “Knowing how to handle a situation...that could save his life,” Christian said.
Christian Campos said his brother, Junior, was in several vehicles that were hit by roadside bombs, and he was shot in the head, but saved by his helmet.
Speaking from North Carolina, Junior said coming back from Afghanistan took some adjustment initially. He had some problems with anger, but not any more.
“I have no issues. I have no problems now,” he said. “I can control my temper now. I’m calm all the time.”
Junior’s looking forward to coming home for Thanksgiving. Christian, is also upbeat about the upcoming visit – but he also plans to spend some time with the “Family of Heroes” program, and go over it with his parents, just in case.
Too little exercise, too much TV tied to depression
Peposted at http://darkestcloset.blogspot.com/ Posted at http://www.reuters.com/article/2011/11/14/us-depression-exercise-idUSTRE7AD04I20111114
Sun Nov 13, 2011 9:26pm EST
(Reuters) - Older women who got more exercise and less television time were the least likely to be diagnosed with depression, according to a U.S. study of thousands of women -- with physical activity having the biggest impact.
According to findings published in the American Journal of Epidemiology, researchers found that women who reported exercising the most in recent years were about 20 percent less likely to get depression than those who rarely exercised.
On the other hand, the more hours they spent watching TV each week, the more their risk of depression crept up.
"Higher levels of physical activity were associated with lower depression risk," wrote study author Michel Lucas, from the Harvard School of Public Health in Boston.
More time spent being active might boost self-esteem and women's sense of control, as well as the endorphins in their blood, although the study could not prove directly that watching too much television and avoiding exercise caused depression, she added.
The report included close to 50,000 women who filled out surveys every couple of years as part of the U.S. Nurses' Health Study, and covered the years 1992 to 2006.
Participants recorded the amount of time they spent watching TV each week in 1992, and also answered questions about how often they walked, biked, ran and swam between 1992 and 2000.
On the same questionnaires, women reported any new diagnosis of clinical depression or medication taken to treat depression.
The analysis only included women who did not have depression in 1996. Over the next decade, there were 6,500 new cases of depression.
After the researchers accounted for aspects of health and lifestyle linked to depression, including weight, smoking and a range of diseases, exercising the most -- 90 minutes or more each day -- meant women were 20 percent less likely to be diagnosed with depression than those who exercised 10 minutes or less a day.
Women who watched three hours or more of television a day were 13 percent more likely to be diagnosed with depression than those who hardly ever tuned in, but Lucas said at least part of that link might be due to women replacing time they could be exercising with TV watching.
One alternative explanation the researchers brought up is that women might have been experiencing some symptoms of depression before they were diagnosed, leading them to exercise less. A formal diagnosis could have come later.
"Previous studies have suggested that physical activity is associated with a lower risk of depressive symptoms," said Gillian Mead, who studies geriatric medicine at Edinburgh's Royal Infirmary but was not involved in the study.
"(The finding) adds to the growing body of evidence that physical activity is important to maintain brain health," she added in an email to Reuters Health. SOURCE: bit.ly/sQbWMU
(Reporting from New York by Genevra Pittman at Reuters Health; editing by Elaine Lies and Ron Popeski)
http://www.reuters.com/article/2011/11/14/us-depression-exercise-idUSTRE7AD04I20111114
Friday, November 11, 2011
Psychiatry manual revisions spark row
US psychiatrists divided by claims of secrecy and scientific overreach.
Reposted at http://wwwdarkestcloset.blogspot.com/
The question of how best to revise the 'bible' of American psychiatry once again has tempers flaring. The manual, the Diagnostic and Statistical Manual of Mental Disorders (DSM), is significant because it is used to determine clinical diagnoses, insurance reimbursements and research agendas throughout the United States, and is often used as a reference in other countries.
Planning for the upcoming fifth edition of the manual (DSM-V) began in 1999, but as work has picked up during the past year, critics have alleged that the process has been too secretive, and that working groups have been pushed to meet an unrealistic 2012 publication date. Some, including the architects behind the last two editions of the DSM, also complain that project leaders are pushing for the premature inclusion of changes meant to incorporate recent genetic and neurobiological advances, before they are ready for the clinic.
Supporters, meanwhile, say that the changes will not be too drastic, and are meant to make the manual more flexible for future revisions.
Even light tweaking of definitions in the DSM can bring about radical changes in psychiatric practice, as Allen Frances, professor emeritus of psychiatry at Duke University in Durham, North Carolina, wrote in a recent commentary in Psychiatric Times. Frances, chairman of the committee that produced the fourth edition of the manual in 1994, acknowledged that changes in the definitions of autistic disorder and attention-deficit/hyperactivity disorder made then may have contributed to the recent surge in diagnoses of these conditions.
In addition, the manual sometimes has an outsized influence on research directions, says Steven Hyman, provost of Harvard University and a member of the DSM-V task force that is overseeing the revision. Hyman became interested in reforming the DSM when he was director of the National Institute of Mental Health in Bethesda, Maryland, and witnessed the control that it exerted over grant review panels. "I was spending taxpayer money on grants that were being forced into categories that might or might not conform to nature," he says.
“There just hasn't been time to do this in an organized way.”
The latest revisions come as financial ties between prominent psychiatrists and pharmaceutical companies are being closely scrutinized. A 2006 analysis of potential conflicts of interest among those who participated in the last revision showed that 56% of panel members had financial links to the pharmaceutical industry (L. Cosgrove et al. Psychother. Psychosom. 75, 154–160; 2006). For the DSM-V, the American Psychiatric Association, which publishes the manual, vetted potential members of working groups under a new conflict-of-interest policy. But the process introduced delays, and working groups were not finalized until 2008.
Then word broke last July that working group members had signed non-disclosure agreements, agreeing to refrain from distributing pre-publication materials or divulging the content of group discussions pertaining to the rewrite. The agreements were intended to prevent members from publishing material to be used in the DSM-V, says Darrel Regier, vice-chair of the DSM-V task force and director of the American Psychiatric Association's research division. But Robert Spitzer, a professor of psychiatry at Columbia University in New York who oversaw the DSM-III, says that his request to look at minutes of a DSM-V meeting was denied because of these confidentiality agreements.Since then, DSM-V working groups have begun posting regular summaries of their activities online. "All of us have been encouraged to be as public as we can be," says William Carpenter of the Baltimore-based University of Maryland School of Medicine and chair of the working group on psychotic disorders. "But just to have [the confidentiality agreements] — that never would have been considered in the previous revisions," says Spitzer.
From the start, Hyman and DSM-V chairman David Kupfer have also planned to change how the DSM-V evaluates mental disorders. Rather than relying strictly on categorical diagnoses — one either has depression or does not, for example — they have pushed to add 'dimensional' criteria to ascertain to what extent a person is depressed. Such criteria could also address similarities among different disorders, reflecting, for example, neuroimaging studies that suggest multiple anxiety disorders can affect the same region of the brain.
For this reason, Carpenter and others have said the DSM-V will represent a "paradigm shift" — an expression that alarmed critics, who say the science behind such dimensional assessments is not yet ready to be incorporated into clinical assessments. In March, Duke University psychologist and epidemiologist Jane Costello resigned from the working group on child and adolescent disorders after receiving a memo from Kupfer and Regier about including the dimensional approach. Adding these assessments would require a great deal of extra research, she says, at a time when working groups were already behind schedule for their 2012 publication deadline. "There just hasn't been time to do this in an organized way," she says. "This is a huge job."
Hyman says that the changes will not necessarily be so drastic, and could take the form of a few additional, and optional, diagnostic criteria without replacing the old methods.
Mental-health guide accused of overreach
Dispute grows over revisions to diagnostic handbook.
Psychologist David Elkins had modest ambitions for his petition. He and his colleagues were worried that proposed changes to an influential handbook of mental disorders could classify normal behaviours as psychological conditions, potentially leading to inappropriate treatments. So they laid out their concerns in an open letter, co-sponsored by five divisions of the American Psychological Association in Washington DC. “I thought, 'Well, maybe we'll get a couple or maybe 30 signatures',” says Elkins, an emeritus professor at Pepperdine University in Malibu, California.
But the letter, posted online on 22 October (http://go.nature.com/uhmvqq), touched a nerve. Within 10 days more than 2,800 people had signed it, many identifying themselves as mental-health professionals.
The petition targets proposed revisions to the Diagnostic and Statistical Manual of Mental Disorders (DSM), a tome used by psychiatrists, psychologists, counsellors and others worldwide to diagnose mental maladies and set research agendas. The American Psychiatric Association, based in Arlington, Virginia, plans to publish a new edition of the manual, DSM-5, in 2013. The association has declined to comment on Elkins's petition.
Elkins's petition is not the first to raise concerns that the DSM-5 proposals could overreach. In June, the British Psychological Society, based in Leicester, issued a critique that highlighted, for example, the proposed addition of 'attenuated psychosis syndrome'. The society argued that this could be used “to stigmatize eccentric people”.
“There should be a black box warning about how child bipolar disorder is being overdiagnosed.”
Efforts to tighten loose definitions of attention deficit and hyperactivity disorder (ADHD) and bipolar disorder in children have also proved controversial. In response to worries that inexact criteria may have contributed to a surge in diagnoses of these conditions since the 1990s, the DSM-5 task force has proposed a syndrome called 'disruptive mood dysregulation disorder', which would provide an alternative to labelling a child as bipolar or having ADHD. But Frances says that is not enough. “There should be a black box warning about how child bipolar disorder is being overdiagnosed,” he says. “Instead, they've created a new disorder.”
Field trials of the proposed DSM-5 criteria have been completed and investigators plan to publish the results. Helena Kraemer, a statistician and emeritus professor at Stanford University School of Medicine in Palo Alto, California, who is on the DSM-5 committee, says that results from trials of some criteria will indicate whether they generate more frequent diagnoses.
But Mojtabai cautions that trial results may not reflect what will happen when DSM-5 is published. “Any trial is artificial,” he says. “The clinicians in these trials have intensive training, but people who will use this manual in clinical practice will not receive that level of instruction.”
- Nature Volume: 479, Pages: 14 ()
Wednesday, October 26, 2011
FDA: Smoking Cessation Drug Does Not Cause More Psychiatric Hospitalizations Than Nicotine Patches
By Join Together Staff | October 25, 2011 |
The Food and Drug Administration (FDA) has determined the smoking cessation drug Chantix (varenicline) is no more likely than nicotine patches to cause psychiatric events that require hospitalization.
The FDA drew its conclusions after reviewing two studies comparing Chantix to nicotine replacement therapy, including nicotine patches. The agency acknowledged the studies had limitations and will keep the “black box” warning labels on Chantix to advise about possible psychiatric side effects, including changes in behavior, hostility, agitation, depressed mood and suicidal thoughts or actions, Reuters reports.
“Overall, FDA has determined that the current warnings in the Chantix drug label, based on postmarketing surveillance reports, remain appropriate,” the FDA said in a statement.
One study conducted by the Department of Veterans Affairs compared 14,131 veterans using Chantix with an equal number of veterans who used nicotine patches. A second study conducted by the Department of Defense compared almost 20,000 people using Chantix with about 16,000 people who used nicotine patches for a month after they began treatment to quit smoking.
The manufacturer of Chantix, Pfizer, is conducting a large safety clinical trial of the drug to assess psychiatric side effects. Results are expected in 2017.
In June, the FDA said Chantix may be associated with a small, increased risk of certain heart problems in patients with heart disease.
http://www.drugfree.org/join-together/research/fda-smoking-cessation-drug-does-not-cause-more-psychiatric-hospitalizations-than-nicotine-patches?utm_source=Join+Together+Daily&utm_campaign=42a2475b68-JT+Daily+News%3A+Take-Back+Programs...&utm_medium=emailReposted at darkestcloset@blogspot.com
Tuesday, October 18, 2011
Health Reform to Increase Number Receiving Medicaid Mental Health Services
The number of Medicaid beneficiaries using mental health and addiction treatment services is expected to increase from 2.1 million in 2006 to 4.4 million in 2019—the date when all health reform provisions are implemented to expand Medicaid coverage to low-income childless adults between the ages of 18 and 64. The number of 18-to-64-year-old adult behavioral health service users overall (counting those covered by Medicare, Medicaid, private insurance, and the uninsured) is expected to increase from 25.4 million in 2006 to 26.6 million by 2019.. The projected increase in behavioral health service utilization was based on research on non-elderly adults’ mental health status and insurance status by income level reported in the 2004–2006 Medical Expenditure Panel Surveys. (Open Minds, 10/10/11)
Monday, October 10, 2011
Happy World Mental Health Day!
World Mental Health Day—October 10, 2011
World Mental Health Day raises public awareness about mental health issues. The day promotes open discussion of mental health and investments in prevention, promotion, and treatment services.This year, the theme is "Investing in Mental Health." Significant behavioral health disparities persist in diverse communities across the globe. To reach these communities, we need to increase investment for mental health and to shift available resources toward more effective forms of services delivered through primary health care and community settings.
Monday, October 3, 2011
Friday, September 30, 2011
My Plan, My Life, My Psychiatric Advance Directive
Similar to a medical advance directive or a health care power of attorney, a psychiatric advance directive is a legal document completed in a time of wellness that provides instructions regarding treatment or services one wishes to have or not have during a mental health crisis, and may help influence his or her care. A mental health crisis is when a person is unable to make or communicate rational decisions.
A psychiatric advance directive allows you to specify considerations about your mental health care treatment and appoint an agent who may make decisions about your treatment in the event of a mental health crisis. In some cases, you may also give further background information about how you have reacted to past treatment.
Despite these benefits, a survey of mental health experts concluded the underuse of psychiatric advance directives in the United States; this study surveyed 1,011 people with serious mental illness receiving public-sector treatment in 5 cities.
On the My Plan, My Life Web site, you will find comprehensive and easy-to-understand information for individuals with mental illness, their families and health care professionals. On the site you can learn about the importance of psychiatric advance directives as a tool for communicating specifics about one’s care during a mental health crisis and how to prepare your own directive.
My Plan, My Life: My Psychiatric Advance Directive is brought to you by Mental Health America and sponsored by Novartis Pharmaceuticals Corporation. http://www.myplanmylife.com/mylife.cfm
Reposted at darkestcloset.bloggerspot
A psychiatric advance directive allows you to specify considerations about your mental health care treatment and appoint an agent who may make decisions about your treatment in the event of a mental health crisis. In some cases, you may also give further background information about how you have reacted to past treatment.
Despite these benefits, a survey of mental health experts concluded the underuse of psychiatric advance directives in the United States; this study surveyed 1,011 people with serious mental illness receiving public-sector treatment in 5 cities.
On the My Plan, My Life Web site, you will find comprehensive and easy-to-understand information for individuals with mental illness, their families and health care professionals. On the site you can learn about the importance of psychiatric advance directives as a tool for communicating specifics about one’s care during a mental health crisis and how to prepare your own directive.
My Plan, My Life: My Psychiatric Advance Directive is brought to you by Mental Health America and sponsored by Novartis Pharmaceuticals Corporation. http://www.myplanmylife.com/mylife.cfm
Reposted at darkestcloset.bloggerspot
Friday, September 23, 2011
Risk for Mental Health Conditions Vary by Gender
Women are more likely to develop anxiety and mood disorders such as depression, while men's mental health issues are more likely to involve antisocial personality and substance use disorders, a new study says. Researchers, whose findings are reported in the Journal of Abnormal Psychology, say the differences are due to the fact that women are more likely to internalize their emotions, which can bring on withdrawal, loneliness and depression, whereas men externalize them, becoming aggressive and impulsive.
Researchers analyzed the answers to interview questions from 43,093 U.S. adults during a 2001 National Institutes of Health survey. For depression, 22.9 percent of women said they had had the condition during their lifetime; 13.1 percent of men said they had. The study showed 7.2 percent of women had panic disorder, and 5.8 percent had generalized anxiety disorder, while just 3.7 and 3.1 percent of men had those conditions, respectively. Among conditions more common in men were alcohol dependence and antisocial personality. (HealthDay News, 8/23/11)
Reposted at darkestcloset.blogspot.com
Researchers analyzed the answers to interview questions from 43,093 U.S. adults during a 2001 National Institutes of Health survey. For depression, 22.9 percent of women said they had had the condition during their lifetime; 13.1 percent of men said they had. The study showed 7.2 percent of women had panic disorder, and 5.8 percent had generalized anxiety disorder, while just 3.7 and 3.1 percent of men had those conditions, respectively. Among conditions more common in men were alcohol dependence and antisocial personality. (HealthDay News, 8/23/11)
Reposted at darkestcloset.blogspot.com
Indonesians with Mental Illness Placed in Cages, Chained
An estimated 30,000 Indonesians with mental illness are placed in cages and chained because of stigma and lack of access to treatment. Last year, the government’s department of mental health announced “Meuju Bebas Pasung,” a roadmap to free people in chains. Although officials have worked to reach communities and raise awareness, the task is difficult because mental health remains low on the government’s list of priorities. (Globalpost, 9/12/11)
Reposted at darkestcloset.bloggerspot.com
Reposted at darkestcloset.bloggerspot.com
People with Depression Don’t Reveal Symptoms to Physicians
People suffering from depression may not bring it up with their doctor for a number of reasons, a study finds. One of the most common reasons is that they are afraid of getting a recommendation for antidepressants.
The study, reported in the journal Annals of Family Medicine, surveyed 1,054 adults about why they wouldn't tell their primary care physician about depression symptoms, as well as their beliefs about the condition. The common reasons reported by participants was the fear of being put on medication, a belief that a doctor isn’t the person to handle such issues, and worries over privacy. At least 10 percent of the participants said that fear of being referred to a counselor or psychiatrist and being branded a psychiatric patient were stumbling blocks. Those who had more barriers to talking to their doctors about depression were likely to be female, Hispanic, with less education and lower income. (Los Angeles Times, 9/12/11)
Reposted at darkestcloset.bloggerspot.com
The study, reported in the journal Annals of Family Medicine, surveyed 1,054 adults about why they wouldn't tell their primary care physician about depression symptoms, as well as their beliefs about the condition. The common reasons reported by participants was the fear of being put on medication, a belief that a doctor isn’t the person to handle such issues, and worries over privacy. At least 10 percent of the participants said that fear of being referred to a counselor or psychiatrist and being branded a psychiatric patient were stumbling blocks. Those who had more barriers to talking to their doctors about depression were likely to be female, Hispanic, with less education and lower income. (Los Angeles Times, 9/12/11)
Reposted at darkestcloset.bloggerspot.com
Study: Suicidal Teens Rarely Receive Treatment
Few suicidal teens receive the treatment and care they need, a new study reports. The researchers found only 13 percent of teenagers with suicidal thoughts visited a mental health professional through their health care network, and only 16 percent received treatment during the year, even though they were eligible for mental health visits without a referral and with relatively low co-payments. In the study, reported in the journal Academic Pediatrics, researchers analyzed the use of health care services among 198 teens ranging in age from 13 to 18 years. Half of the teenagers had had suicidal thoughts; the other half did not. The researchers found mental health services were underused among all of the teens studied. Although 86 percent of the teens with suicidal thoughts had seen a health care provider, only 13 percent had seen a mental health specialist. Just 7 percent received antidepressants, the study found. (HealthDay News, 9/16/11)
Reposted at darkestcloset.blogspot.com
Reposted at darkestcloset.blogspot.com
Thursday, September 22, 2011
Madness in the NFL - The Greg Montgomery Story
“Madness in the NFL - The Greg Montgomery Story” documentary takes us on Greg's journey from All-Pro NFL punter to his diagnosis with bipolar disorder in 1997 while playing with the Baltimore Ravens. Ultimately, his journey towards recovery from bipolar disorder has been a positive and successful one. Now almost 14 years after his diagnosis of bipolar disorder, Greg is a powerful advocate in the field of mental health. He recognizes that help is desperately needed for the millions living with mental illness and is making a difference by speaking out.
Greg is also an avid writer and blogger. Through his blog, Zen In The Art of Living Bipolar, Greg openly shares his experiences of anxiety, depression and bipolar disorder with educational, honest, and engaging content. You can also follow Greg on Twitter @ZenPunter.We commend Greg for his advocacy efforts and for working with numerous mental health organizations on raising awareness and fighting the stigma that surrounds mental illness. DBSA looks forward to partnering with him on these upcoming DBSA initiatives:
- The October eUpdate will feature an empowering article written by Greg.
- In November, DBSA will host a live Telechat with Greg. Stay tuned for more information and how you can submit your questions in advance.
Reposted at darkestcloset.blogspot.com
Laughter Really Is the Best Medicine, Study Suggests
Having a good laugh with friends helps people deal with pain, a new study suggests. An international research team, led by Oxford University, found that real laughter triggers the release of protective endorphins, which manage pain and promote feelings of well being.
According to the team’s research, published online in Proceedings of the Royal Society B, watching just 15 minutes of comedy with others increased the pain threshold by an average of about 10 per cent. The fact that only hearty, rather than polite, laughter releases endorphins has probably evolved as a way of promoting socializing among humans, the researchers suggest. Many studies have already shown that laughter is 30 times more likely to occur if people are together rather than alone. The endorphin rush appears to be limited to a good belly laugh, shared with others. The paper distinguishes between unforced laughter and polite laughter. It concludes that when we laugh hard we produce a series of exhalations without drawing breath, an involuntary physical mechanism that is limited to humans and appears to trigger the release of endorphins.
Source: http://www.ox.ac.uk/media/news_stories/2011/111409_1.html
According to the team’s research, published online in Proceedings of the Royal Society B, watching just 15 minutes of comedy with others increased the pain threshold by an average of about 10 per cent. The fact that only hearty, rather than polite, laughter releases endorphins has probably evolved as a way of promoting socializing among humans, the researchers suggest. Many studies have already shown that laughter is 30 times more likely to occur if people are together rather than alone. The endorphin rush appears to be limited to a good belly laugh, shared with others. The paper distinguishes between unforced laughter and polite laughter. It concludes that when we laugh hard we produce a series of exhalations without drawing breath, an involuntary physical mechanism that is limited to humans and appears to trigger the release of endorphins.
Source: http://www.ox.ac.uk/media/news_stories/2011/111409_1.html
MacArthur “Genius” Awards Include Grant to Suicide and Self-Injury Researcher
Matthew Nock, a Harvard University psychology professor studying suicide prevention, has received a MacArthur Fellowship, which includes a no-strings-attached grant of $500,000 ($100,000 annually for five years). The fellowships, popularly known as the “genius” awards, were announced on September 20 by the John D. and Catherine T. MacArthur Foundation.
Most recently, Nock’s research has identified a behavioral marker that might help predict suicide attempts. His research indicates that individuals who are suicidal react differently than non-suicidal people when they see words such as “suicide” or “death” on the monitor during a computer game. Seeing these words “captures their thinking and slows down their response,” Nock told The Los Angeles Times. “It’s an objective marker. It doesn’t require them to tell you whether they are suicidal.” At the same time, a recent study – published in Academic Pediatrics – has found that suicidal teens are not likely to get the mental health care they need. Among other findings, the researchers found that when all types of mental health services were combined (including antidepressants and care received through outside sources), only 26 percent of teens with suicidal ideation in the study received services the previous year.
Sources: http://www.latimes.com/health/boostershots/la-heb-macarthur-suicide-20110920,0,2354849.story
http://www.eurekalert.org/pub_releases/2011-09/sc-sfo091311.php
Reposted at darkestcloset.blogspot.com
Most recently, Nock’s research has identified a behavioral marker that might help predict suicide attempts. His research indicates that individuals who are suicidal react differently than non-suicidal people when they see words such as “suicide” or “death” on the monitor during a computer game. Seeing these words “captures their thinking and slows down their response,” Nock told The Los Angeles Times. “It’s an objective marker. It doesn’t require them to tell you whether they are suicidal.” At the same time, a recent study – published in Academic Pediatrics – has found that suicidal teens are not likely to get the mental health care they need. Among other findings, the researchers found that when all types of mental health services were combined (including antidepressants and care received through outside sources), only 26 percent of teens with suicidal ideation in the study received services the previous year.
Sources: http://www.latimes.com/health/boostershots/la-heb-macarthur-suicide-20110920,0,2354849.story
http://www.eurekalert.org/pub_releases/2011-09/sc-sfo091311.php
Reposted at darkestcloset.blogspot.com
Mental Health Reporting Website Educates Journalists
The University of Washington offers a website to educate journalists on how to report on stories that involve mental health issues. The site, at the source below, provides information including a “Checklist for Reporting on Mental Illness.” The checklist urges journalists to “[w]rite with awareness that people with mental illness face prejudice and discrimination,” and “[a]void using language that implies people with mental illness are violent,” among other suggestions.
Source: http://depts.washington.edu/mhreport/ reposted at darkestcloset.bloggerspot.com
http://depts.washington.edu/mhreport/
Source: http://depts.washington.edu/mhreport/ reposted at darkestcloset.bloggerspot.com
http://depts.washington.edu/mhreport/
Deadlines Approach for Four Webinars
Four webinars – on “Demystifying Trauma,” “Working with Voices,” Starting a Peer-Run Respite, and Coalition-Building, respectively – will take place next week! “Demystifying Trauma: Sharing Pathways to Healing and Wellness,” organized by SAMHSA’s ADS Center (Resource Center to Promote Acceptance, Dignity and Social Inclusion Associated with Mental Health), will take place Sept. 26, 2011, 3 p.m. – 4:30 p.m. ET. Registration closes at 5 p.m. ET on Sept. 25. To register, click on the following link: http://promoteacceptance.samhsa.gov/teleconferences/archive/training/teleconference09262011.aspx.
“Working with Voices” will focus on the Hearing Voices Network and Hearing Voices Groups, which do not pathologize hearing voices or other altered experiences. It will take place Sept. 27, 1 p.m. – 2:30 p.m. ET. Space is limited; to register, click here: http://cts.vresp.com/c/?NationalMentalHealth/14baa0ba54/ac1ab23981/db99ce0be4. “So You Want to Start a Peer-Run Respite?” will take place on Sept. 28, 1 p.m. – 2:30 p.m. ET. It the first webinar in a peer-run respite series sponsored by the National Empowerment Center. Space is limited; registration will close on Sept. 27.
To register, click here: https://www3.gotomeeting.com/register/728369694.
“Coalition Building 101 for Mental Health Consumers and Psychiatric Survivors: Finding Common Ground with Each Other and Allies,” to be held Sept. 30, 2:00 p.m. – 3:30 p.m. ET, will include how to address obstacles to sustaining a coalition, action steps to build and/or sustain a coalition, what to do when groups may be competing for the same resources, and more!
To register, e-mail rsvppeerlink@gmail.com with “Coalition Building” in the subject line
Sources: http://promoteacceptance.samhsa.gov
http://www.nyaprs.org
http://www.power2u.org
SAMHSA/CMHS Consumer Affairs E-News, September 20, 2011
“Working with Voices” will focus on the Hearing Voices Network and Hearing Voices Groups, which do not pathologize hearing voices or other altered experiences. It will take place Sept. 27, 1 p.m. – 2:30 p.m. ET. Space is limited; to register, click here: http://cts.vresp.com/c/?NationalMentalHealth/14baa0ba54/ac1ab23981/db99ce0be4. “So You Want to Start a Peer-Run Respite?” will take place on Sept. 28, 1 p.m. – 2:30 p.m. ET. It the first webinar in a peer-run respite series sponsored by the National Empowerment Center. Space is limited; registration will close on Sept. 27.
To register, click here: https://www3.gotomeeting.com/register/728369694.
“Coalition Building 101 for Mental Health Consumers and Psychiatric Survivors: Finding Common Ground with Each Other and Allies,” to be held Sept. 30, 2:00 p.m. – 3:30 p.m. ET, will include how to address obstacles to sustaining a coalition, action steps to build and/or sustain a coalition, what to do when groups may be competing for the same resources, and more!
To register, e-mail rsvppeerlink@gmail.com with “Coalition Building” in the subject line
Sources: http://promoteacceptance.samhsa.gov
http://www.nyaprs.org
http://www.power2u.org
SAMHSA/CMHS Consumer Affairs E-News, September 20, 2011
Sunday, September 11, 2011
Does cutting mental health care increase the prison population?
The Washington Post, Suzy Khimm, 06/02/2011 Reposted at darkestcloset.bloggerspot.com
State-supported mental health care, like many social services, has been especially vulnerable in the recent rounds of budget cuts. Over the past two years, some $1.6 billion has been slashed from non-Medicaid state spending on mental health, according to the National Alliance on Mental Illness. But a growing number of law enforcement officials - along with mental health advocates - are voicing concerns that such cutbacks not only hurt mental health beneficiaries but also overburden the country's prison system.
State-supported mental health care, like many social services, has been especially vulnerable in the recent rounds of budget cuts. Over the past two years, some $1.6 billion has been slashed from non-Medicaid state spending on mental health, according to the National Alliance on Mental Illness. But a growing number of law enforcement officials - along with mental health advocates - are voicing concerns that such cutbacks not only hurt mental health beneficiaries but also overburden the country's prison system.
Time Magazine Zeroes In on Horrific Abuse in Residential Care
An investigative reporter at a major news weekly recently published a blueprint for preventing the terrible abuse and neglect that routinely occur in institutions that are supposed to serve individuals with disabilities. Citing investigations by The New York Times and the Miami Herald, which uncovered ongoing violations – including those leading to deaths – in such institutions, Time magazine’s Maia Szalavitz came up with a template for putting an end to such abuse. Her suggestions include intensive oversight and “redundant checks on power,” frequent and unannounced inspections, a reduction in stigma, and adequate funding. “If we want the elderly, disabled and others living in institutions to be safe and well cared for, we need to value them both emotionally and financially,” Szalavitz writes. “That’s not what’s going on now.”
Source: http://healthland.time.com/2011/06/07/why-so-much-abuse-is-allowed-to-continue-in-residential-care/ Reposted at darkestcloset.bloggerspot.com
Source: http://healthland.time.com/2011/06/07/why-so-much-abuse-is-allowed-to-continue-in-residential-care/ Reposted at darkestcloset.bloggerspot.com
Study Notes High Prevalence of Alcohol Dependency Among Adults with Psychiatric Disabilities
A new nationwide survey has revealed that adults diagnosed with mental illnesses are four times more likely to develop alcohol dependency than adults who do not have such a diagnosis (9.6 percent compared to 2.2 percent), according to the Substance Abuse and Mental Health Services Administration (SAMHSA). The rate of alcohol dependency increases as the severity of the mental illness increases, the report found. “This SAMHSA study adds to the evidence” of the connection between mental health and substance use disorders, said SAMHSA administrator Pam Hyde. The full report is available at http://oas.samhsa.gov/spotlight/Spotlight027AlcoholDependence.pdf. For related publications and information, visit http://www.samhsa.gov/.
Source: http://www.samhsa.gov
Source: http://www.samhsa.gov
What mom thinks matters
Fred Markowitz
Attitudes of family members can impede recovery from mental illness
DeKalb, Ill. – A new study led by a Northern Illinois University sociologist shows that while family members often provide critical support, they also can sometimes be the source of stigmatizing attitudes that impede the recovery of mentally ill relatives.
“Negative attitudes of family members have the potential to affect the ways that mentally ill persons view themselves, adversely influencing the likelihood of recovery from the illness,” said lead researcher Fred Markowitz, an NIU professor of sociology.
Markowitz and his colleagues, Beth Angell from Rutgers and Jan Greenberg from the University of Wisconsin-Madison, published their findings in the June issue of Social Psychology Quarterly, a peer-reviewed journal of the American Sociological Association.
Over an 18-month period, the researchers studied 129 mothers of adult children with schizophrenia.
“In short, what mom thinks matters,” Markowitz said. “It’s a chain of effects that unfolds.
“We found that when those with mental illness exhibited greater levels of initial symptoms, lower self-confidence and quality of life, their mothers tended to view them in more stigmatized terms—for example, seeing them as ‘incompetent,’ ‘unpredictable’ and ‘unreliable,’ ” Markowitz said. “When mothers held these views, their sons and daughters with mental illness were more likely to come to see themselves in similar terms—what social psychologists call ‘the reflected appraisals process.’ Importantly, when the individuals with mental illness took on these stigmatizing views of themselves, their symptoms became somewhat greater and levels of self-confidence and quality of life lower.”
A long line of research has shown that the stigma associated with mental illness can be a major impediment to recovery, affecting self-esteem and even job prospects. But research has not historically examined the links between stigma, reflected appraisals, identity formation and recovery, Markowitz said.
“Our study is part of research that is starting to more fully examine how stigma affects the self-concept and identity of those with mental illness,” he said.
Markowitz and his colleagues believe it is important to acknowledge that many of the sentiments conveyed toward ill relatives grow out of positive intentions and reflect attempts to cope with the difficulties of having a relative with serious mental illness. Yet, stigmatizing attitudes are of concern because of their potential adverse effects.
“This study highlights the notion that recovery from mental illness is not simply a matter of controlling symptoms as indicated by a strictly ‘psychiatric’ perspective,” Markowitz said. “It is, to a certain extent, a social-psychological process.
“The ways in which people, including family members and service providers, think about persons with mental illness affect the beliefs and actions of the individuals with mental illness, in turn shaping the trajectory of recovery.”
DeKalb, Ill. – A new study led by a Northern Illinois University sociologist shows that while family members often provide critical support, they also can sometimes be the source of stigmatizing attitudes that impede the recovery of mentally ill relatives.
“Negative attitudes of family members have the potential to affect the ways that mentally ill persons view themselves, adversely influencing the likelihood of recovery from the illness,” said lead researcher Fred Markowitz, an NIU professor of sociology.
Markowitz and his colleagues, Beth Angell from Rutgers and Jan Greenberg from the University of Wisconsin-Madison, published their findings in the June issue of Social Psychology Quarterly, a peer-reviewed journal of the American Sociological Association.
Over an 18-month period, the researchers studied 129 mothers of adult children with schizophrenia.
“In short, what mom thinks matters,” Markowitz said. “It’s a chain of effects that unfolds.
“We found that when those with mental illness exhibited greater levels of initial symptoms, lower self-confidence and quality of life, their mothers tended to view them in more stigmatized terms—for example, seeing them as ‘incompetent,’ ‘unpredictable’ and ‘unreliable,’ ” Markowitz said. “When mothers held these views, their sons and daughters with mental illness were more likely to come to see themselves in similar terms—what social psychologists call ‘the reflected appraisals process.’ Importantly, when the individuals with mental illness took on these stigmatizing views of themselves, their symptoms became somewhat greater and levels of self-confidence and quality of life lower.”
A long line of research has shown that the stigma associated with mental illness can be a major impediment to recovery, affecting self-esteem and even job prospects. But research has not historically examined the links between stigma, reflected appraisals, identity formation and recovery, Markowitz said.
“Our study is part of research that is starting to more fully examine how stigma affects the self-concept and identity of those with mental illness,” he said.
Markowitz and his colleagues believe it is important to acknowledge that many of the sentiments conveyed toward ill relatives grow out of positive intentions and reflect attempts to cope with the difficulties of having a relative with serious mental illness. Yet, stigmatizing attitudes are of concern because of their potential adverse effects.
“This study highlights the notion that recovery from mental illness is not simply a matter of controlling symptoms as indicated by a strictly ‘psychiatric’ perspective,” Markowitz said. “It is, to a certain extent, a social-psychological process.
“The ways in which people, including family members and service providers, think about persons with mental illness affect the beliefs and actions of the individuals with mental illness, in turn shaping the trajectory of recovery.”
Subscribe to:
Comments (Atom)